Clinical
What to prescribe for myopia control
In this article:
The efficacy of myopia control treatments and how to select the ideal option(s) for your patient are described here, with the support of the free-to-download, multi-language Managing Myopia Guidelines Infographic. These infographics can be used both as a chairside reference and to support clinical communication with patients and their parents or carers. The evidence base for understanding efficacy and prescribing considerations are detailed.
- Q1: What is the most effective treatment that you have available to you?
- Q2: Spectacles or contact lenses?
- Q3: Which contact lens option suits best?
- Q4: Is binocular vision function normal?
- Q5: How about prescribing atropine?
- The full picture on what to prescribe
- The Managing Myopia Guidelines Infographics
There is no one-size-fits-all prescribing choice with myopia management, so which option should you choose for your individual patient? Here we are going to ask you to consider fivekey clinical questions in selecting an option for myopia management.
The Managing Myopia Guidelines Infographics are a free-to-download clinical resource designed by Myopia Profile to support clinical decision making and communication. Half of the infographic is a chair-side reference (below left - the mostly blue-coloured panels) and half is to guide in-room discussions with patients and parents (multi-coloured panels, below right). The red boxes highlight the panels which you can utilize together to consider your prescribing choice and then make recommendations, supported by this resource.
We’ll focus on the blue-coloured panel first - the chairside reference to guide your prescribing recommendations. The first of your five clinical questions is as follows.
Q1: What is the most effective treatment that you have available to you?
The multi-coloured panel highlighted on the right provides a summary of treatment options based on current understanding of efficacy. Many treatments appear to offer similar efficacy to slow myopia progression, with no single treatment showing clear superiority.1,2
The podium presentation of treatments below takes into consideration the outcomes of randomized controlled trials of myopia control treatments where there is at least 12 months of data published. It also utilizes axial length data, which is much more accurate than refraction in gauging myopia control success and is a necessity to understand efficacy from a myopia control study. While percentages reported in a single study are useful to understand how well that treatment works compared to the control group, the percentage only applies to that study and cannot be compared directly to other studies.1
Instead of directly comparing percentages from study-to-study, the podium presentation shown below considers percentages as simplified categories, where the research has shown that particular treatment to effectively slow axial elongation by at least 50% or around 33%, give-or-take. We can then communicate these to parents and set treatment goals based on average outcomes for that treatment being to slow myopia progression by "at least half" for the 50% category and "about a third" for the 33% category. Learn more about all of these in our article Which myopia control treatment works best?
The myopia control treatments sitting on the ‘best’ podium have been shown to reduce axial length progression by around 50%, give or take, compared to the single vision control group in each study. In the 'best options' category from left-to-right are atropine 0.05%,3 dual-focus soft contact lens (CooperVision MiSight 1 day),4 and orthokeratology.5
The next row shows the new generation of myopia controlling spectacle lenses with lenslets or diffusion technology. The spectacle lens graphics pictured here, left-to-right, are DIMS Technology (Hoya MiYOSMART),6 H.A.L.T. Technology (Essilor Stellest),7 and Diffusion Optics Technology or DOT (SightGlass DOT lens).8 They all appear to have similar efficacy based on their one-year randomized controlled trial studies.
A new non co-axial ring-focus soft contact lens design (Johnson & Johnson Acuvue Abiliti 1-Day)9 has published six month data which looks like it is heading for the gold podium, once 12 month data is published. Additionally, a randomized controlled trial of an extended-depth-of-focus multifocal contact lens (Visioneering Technologies NaturalVue Multifocal 1 Day) is underway, with preliminary 12 month data indicating a gold podium finish is in sight.
The advantage of this comparison method is that it is evidence-based, easy to understand and explain, and gives you as the practitioner multiple prescribing options in the 'best' and the 'next-best' categories. Note that not all of these myopia control treatment options are available in all countries.
Your first consideration is prescribing an effective spectacle or contact lens option, which offers the dual benefit of myopia correction and myopia control. Select from the best (gold podium) of treatments where possible. Get more guidance on how to describe this to patients and their parents in our article Keys to communication in myopia management.
Q2: Spectacles or contact lenses?
If you are fortunate enough to have access to both spectacle and contact lens options from the ‘best’ treatment options podium, the next question is - spectacles or contact lenses? You have to correct the myopia so it makes sense, where possible, to prescribe a first line treatment which both corrects and controls myopia. Choosing between spectacles and contact lenses for a child is most likely dependent on personal preference, lifestyle, and accessibility to specific products.
If the choice is a spectacle lens option, jump straight to Q4 for binocular vision considerations. If choosing the contact lens route, move to Q3 to narrow down to the contact lens options.
Q3: Which contact lens option suits best?
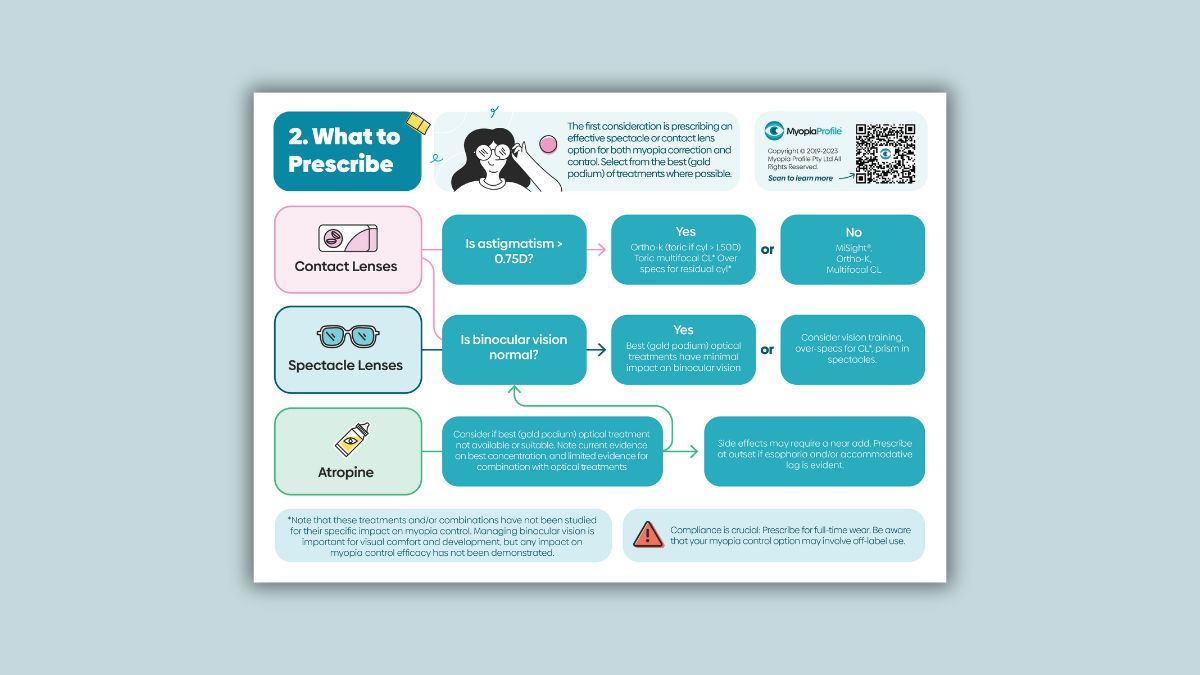
The child’s preference and lifestyle may have already guided you to the most suitable contact lens modality. However, this may be restricted by their refraction. Level of astigmatism is a key differentiator in prescribing myopia control contact lens options. The image below is a section of the Myopia Management Guidelines Infographic chairside reference panel entitled ‘What to prescribe’.
Correcting astigmatism exceeding 0.75D is important as without doing so may under correct the child, potentially fuelling more myopic progression.10 Undercorrection of astigmatism can also negatively impact acuity and academic-related performance at school.11
If astigmatism exceeds 0.75D, ortho-k could be suitable. Read more in our article Who are ideal candidates for orthokeratology? Toric orthokeratology is just as effective for myopia control as spherical fits.12 While toric multifocal soft contact lenses are available, they have not been studied for myopia control: the spherical Biofinity Multifocal centre distance with +2.50 Add has shown efficacy.13 Clinical reports of prescribing spectacles with residual astigmatism correction for use over the top of spherical myopia control soft contact lenses have occured, but have not been studied for efficacy - compliance in these cases would be crucial to avoid undercorrection.
If astigmatism does not exceed 0.75D, ortho-k and various soft myopia control contact lenses should be suitable, in line with the participant characteristics in those clinical trials.4,9,13
Including patients and their parents in the decision making process is vital to ensure motivation and compliance. You can download and print the My Kids Vision QR code sheet, which connects parents with specific information based on your discussions. These link to specific articles on MyKidsVision.org such as Which is the best option for myopia control? to support your communication and give parents further information on your recommendations.
Q4: Is binocular vision function normal?
The image below shows another section of the Myopia Management Guidelines Infographic chairside reference panel entitled ‘What to prescribe’. In children with normal vergence and accommodative function, the best (gold podium) spectacle and contact lens treatments should not impact binocular vision. In children with binocular vision dysfunctions requiring active management, the myopia control treatment may need to be considered separate to the binocular vision treatment.
Managing binocular vision conditions are important to a child's ability to comfortably read, learn and participate in daily activities. While there is a long research history linking specific binocular vision disorders, we cannot state with certainty that fixing a BV dysfunction will lead to a specific myopia control effect.14
Some studies have suggested that myopia control efficacy may vary depending on accommodative and vergence. Children with lower accommodative amplitude appear to benefit the most from orthokeratology,15 while accurate accommodation seems important for efficacy in multifocal soft contact lenses.16 Progressive additional lenses may be the ideal prescribing choice for children with higher accommodative lag and near esophoria, and while this may manage bincoular vision dysfunction, there will only be a small myopia control effect.17,18 Myopia controlling spectacle lens designs like DIMS and H.A.L.T technology provide the highest levels of efficacy, but the lenslets do not function as an ‘add’ to alter binocular vision function.6,7 For more information, read our article Four reasons why binocular vision matters in myopia management.
Q5: How about prescribing atropine?
The image below shows another section of the Myopia Management Guidelines Infographic chairside reference panel entitled ‘What to prescribe’. You'll notice low-concentration atropine is mentioned here as a first line monotherapy treatment if the equivalent optical treatments are not available or suitable. Based on current evidence, atropine 0.05% sits on the ‘best’ podium alongside the best performing spectacle and contact lens treatments.
You may consider including atropine as a first line combination therapy with a spectacle or contact lens option for a child with a number of risk factors for faster progression (eg. younger current age, two myopic parents). Note that there is only conclusive research evidence for combining 0.01% atropine with orthokeratology at this stage to boost efficacy. Early data for the combination of atropine 0.01% and DIMS spectacle lenses shows promise, while a limited clinical data analysis did not show the same for MiSight 1 day contact lenses. Atropine 0.01% added to Biofinity Multifocal CD +2.50 Add soft contact lenses did not reach a significant ‘boost’ effect for efficacy in a three year randomized controlled trial.
In considering binocular vision function (the final box in the image above), a child with esophoria and accommodative lag at baseline may show exacerbation with atropine treatment, so consider if a near add is required in these cases.
Compliance is crucial to myopia control success. Whatever treatment option is selected, prescribe it for full-time wear and/or every day use. In published studies, this means at least 12 hours per day, 7 days per week for spectacles7 and 6 to 7 days per week for contact lenses.4
The full picture on what to prescribe
The image below is the full chairside reference panel for the Managing Myopia Guidelines Infographic providing guidance on what to prescribe. Presuming your knowledge of myopia control treatment efficacy, you will have firstly kept in mind what you have available to you. What will likely best suit the patient then comes down to the variety of factors described here: spectacles versus contact lenses, their refraction, binocular vision function and risk factors for fast myopia progression. Personal and family preferences are also crucial to consider to ensure best outcomes for the patient.
There are numerous 'correct' myopia control options for your patient, since many have similar efficacy: choose the ideal treatment based on what you have available and what best suits their ocular, lifestyle and family factors.
The Managing Myopia Guidelines Infographics
Myopia Profile’s popular and entirely free Managing Myopia Guidelines Infographics are designed to support clinical communication and decision making in myopia management. These engaging infographics are available to download and print in several formats and numerous language translations.
There are two four-panel infographics which can be printed in large format as poster (ANSI-C or A2), or scaled down to US Letter or A4 to be used as a handheld infographic for in-room discussions and reference.
The mostly blue infographic is a chairside reference guide for eye care professionals that guides you through: (1) Myopia risk factors, (2) What to prescribe, (3) Follow-up schedules and (4) Gauging success
The multi-colored infographic is designed to help you communicate with parents and patients on the following topics : (1) Visual environment advice, (2) What are my options? (3) Kids can wear contact lenses and (4) Why myopia management is essential.
The Infographics can also be printed as individual panels (US Letter and A4 sizes) to use each page on its own if you prefer. As above, there are four which are parent- and patient-facing (multi-coloured) and four which are your chairside reference (mostly blue coloured). The image below shows various print formats, with all panels collated (at back) and single pages (foreground).
Freshly updated in late 2023 and built from the ground up from continued feedback with eye care practitioners and industry advisers, these Managing Myopia Guidelines Infographics are designed to be used by eye care professionals, in discussion with patients and their carers, and as a clinical reference.
For an overview of how to use the Infographics in practice, read our article Using the Managing Myopia Guidelines Infographics
For guidance on the guided clinical communication process provided the Infographics, read our article Keys to Communication in Myopia Management.
Once you have used the Infographics to explain myopia to patients and their parents or carers in your exam room, these messages can be further enhanced by providing the take-home, free-to-download Managing Myopia patient brochure.
If you're not too confident in binocular vision, our comprehensive, self-paced online course Binocular Vision Fundamentals is specifically designed to help you increase your skills and clinical scope in binocular vision management. This course is relevant to management of patients of all ages, not just myopes, and you can try the first two lessons for free. There's also free resources to help you upskill in binocular vision on our YouTube channel.
Meet the Authors:

About Kate Gifford
Dr Kate Gifford is an internationally renowned clinician-scientist optometrist and peer educator, and a Visiting Research Fellow at Queensland University of Technology, Brisbane, Australia. She holds a PhD in contact lens optics in myopia, four professional fellowships, over 100 peer reviewed and professional publications, and has presented almost 300 conference lectures around the world. Kate is the Chair of the Clinical Management Guidelines Committee of the International Myopia Institute. In 2016 Kate co-founded Myopia Profile with Dr Paul Gifford; the world-leading educational platform on childhood myopia management. After 13 years of clinical practice ownership, Kate now works full time on Myopia Profile.

About Kimberley Ngu
Kimberley is a clinical optometrist from Perth, Australia, with experience in patient education programs, having practiced in both Australia and Singapore.
Read Kimberley's work in many of the case studies published on MyopiaProfile.com. Kimberley also manages our Myopia Profile and My Kids Vision Instagram and My Kids Vision Facebook platforms.
References
Brennan NA, Toubouti YM, Cheng X, Bullimore MA. Efficacy in myopia control. Prog Retin Eye Res. 2021 Jul;83:100923.
Gifford P, Gifford KL. Descriptive statistical comparison of interventions for myopia control. Invest Ophthalmol Vis Sci 2023;64:822.
Yam JC, Jiang Y, Tang SM, Law AKP, Chan JJ, Wong E, Ko ST, Young AL, Tham CC, Chen LJ, Pang CP. Low-Concentration Atropine for Myopia Progression (LAMP) Study: A Randomized, Double-Blinded, Placebo-Controlled Trial of 0.05%, 0.025%, and 0.01% Atropine Eye Drops in Myopia Control. Ophthalmology. 2019 Jan;126(1):113-124.
Chamberlain P, Peixoto-de-Matos SC, Logan NS et al. A 3-Year Randomized Clinical Trial of Misight Lenses for Myopia Control. Optom Vis Sci 2019;96:556-67.
Sun Y, Xu F, Zhang T, Liu M, Wang D, Chen Y, Liu Q. Orthokeratology to control myopia progression: a meta-analysis. PLoS One. 2015 Apr 9;10(4):e0124535.
Lam CSY, Tang WC, Tse DY et al. Defocus Incorporated Multiple Segments (DIMS) Spectacle Lenses Slow Myopia Progression: A 2-Year Randomised Clinical Trial. Br J Ophthalmol 2020;104:363-8.
Bao J, Huang Y, Li X, Yang A, Zhou F, Wu J, Wang C, Li Y, Lim EW, Spiegel DP, Drobe B, Chen H. Spectacle Lenses With Aspherical Lenslets for Myopia Control vs Single-Vision Spectacle Lenses: A Randomized Clinical Trial. JAMA Ophthalmol. 2022 May 1;140(5):472-478.
Rappon J, Chung C, Young G, Hunt C, Neitz J, Neitz M, Chalberg T. Control of myopia using diffusion optics spectacle lenses: 12-month results of a randomised controlled, efficacy and safety study (CYPRESS). Br J Ophthalmol. 2022 Sep 1:bjophthalmol-2021-321005.
Cheng X, Xu J, Brennan NA. Randomized trial of soft contact lenses with novel ring focus for controlling myopia progression. Ophthalmol Sci 2022:Oct 18.
Yazdani N, Sadeghi R, Ehsaei A, Taghipour A, Hasanzadeh S, Zarifmahmoudi L, Heravian Shandiz J. Under-correction or full correction of myopia? A meta-analysis. J Optom. 2021 Jan-Mar;14(1):11-19.
Narayanasamy S, Vincent SJ, Sampson GP, Wood JM. Simulated astigmatism impairs academic-related performance in children. Ophthalmic Physiol Opt. 2015 Jan;35(1):8-18.
Chen C, Cheung SW, Cho P. Myopia control using toric orthokeratology (TO-SEE study). Invest Ophthalmol Vis Sci. 2013 Oct 3;54(10):6510-7
Walline JJ, Walker MK, Mutti DO, Jones-Jordan LA, Sinnott LT, Giannoni AG, Bickle KM, Schulle KL, Nixon A, Pierce GE, Berntsen DA; BLINK Study Group. Effect of High Add Power, Medium Add Power, or Single-Vision Contact Lenses on Myopia Progression in Children: The BLINK Randomized Clinical Trial. JAMA. 2020 Aug 11;324(6):571-580.
Logan NS, Radhakrishnan H, Cruickshank FE, Allen PM, Bandela PK, Davies LN, Hasebe S, Khanal S, Schmid KL, Vera-Diaz FA, Wolffsohn JS. IMI Accommodation and Binocular Vision in Myopia Development and Progression. Invest Ophthalmol Vis Sci. 2021 Apr 28;62(5):4.
Zhu M, Feng H, Zhu J, Qu X. The impact of amplitude of accommodation on controlling the development of myopia in orthokeratology. Zhonghua Yan Ke Za Zhi. 2014; 50: 14–19.
Cheng X, Xu J, Brennan NA. Accommodation and its role in myopia progression and control with soft contact lenses. Ophthalmic Physiol Opt. 2019 May;39(3):162-171.
Gwiazda JE, Hyman L, Norton TT, et al. Accommodation and related risk factors associated with myopia progression and their interaction with treatment in COMET children. Invest Ophthalmol Vis Sci. 2004; 45: 2143–2151.
Berntsen DA, Sinnott LT, Mutti DO, Zadnik K. A randomized trial using progressive addition lenses to evaluate theories of myopia progression in children with a high lag of accommodation. Invest Ophthalmol Vis Sci. 2012 Feb 13;53(2):640-9.
Enormous thanks to our visionary sponsors
Myopia Profile’s growth into a world leading platform has been made possible through the support of our visionary sponsors, who share our mission to improve children’s vision care worldwide. Click on their logos to learn about how these companies are innovating and developing resources with us to support you in managing your patients with myopia.