Clinical
A Novel Soft Radial Refractive Gradient (SRRG) contact lens for myopia control
In this article:
Recently, I completed my PhD on myopia control with a soft Radial Refractive Gradient (RRG) design contact lens. This experimental design was primarily based on the peripheral retinal blur theory, that E. Smith developed,1 providing an incremental, progressive, refractive change from the central visual axis to peripheral retina, reaching a +2.00D add plus power at about 35 degrees of retinal eccentricity and achieving about +6.00D of addition plus power at the edge of the optical zone (4mm semichord diameter). Our results were similar to other investigations with a myopia controlling effect of 43% on refractive change and 27% on Axial Length (AL) growth, compared to a Single Vision spectacle wearing Group. Moreover, we compared with a concurrent orthokeratology (OK) group, who obtained a 67% refractive and a 38% AL reduction in myopia progression for the two years of the study. Interestingly, this was not statistically different to the RRG design, meaning that this kind of "anti-myopia" lens has a myopia control effectivity similar to OK. This has huge clinical implications, since not all refractions, kids or parents are willing to undertake an orthokeratology process, and it is necessary to have alternatives that may maintain myopia at lower levels where contact lens wearing risk and association with future myopic ocular pathologies are lower. A link to my recent publication in the open access journal BioMed Research International is here.
After analyzing these results, many questions arise in attempts to understand the causes and mechanisms leading to myopia. The issue is that by increasing the peripheral plus power on a contact lens or performing orthokeratology we simultaneously modify several optical aspects. We change relative peripheral refraction, off-axis astigmatism, higher order optical aberrations, lag of accommodation, contrast sensitivity and more.
Because the peripheral retina is much bigger in surface area than central fovea, its importance in the process of visual development seems logical. We know that when an eye receives two different images of focus, it tends to use the one that is in front of the retina. Many mechanisms, not yet well understood, are active - for example, we can measure a choroidal thickness increase that temporarily reduces Axial Length2,3. The majority of studies use an autorefractor to measure relative peripheral refractive error and account for the spherical equivalent value (M), which in reality is a huge limitation on what is really happening with the peripheral image. Images are formed by all the light that passes through the pupil - a cone rather than a beam of light - and includes all aberrations, not only sphere and cylinder. The main aberration affecting peripheral refraction is oblique astigmatism.
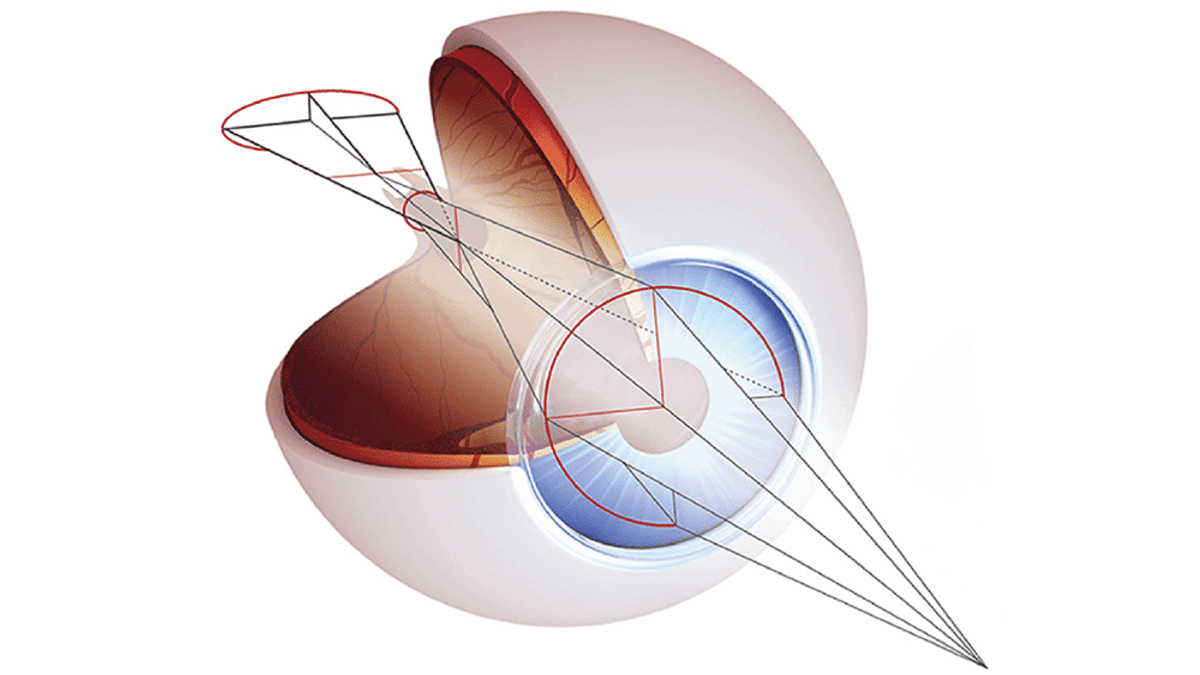
Any optical system suffers from high values of oblique astigmatism when light goes off axis. In the case of the human eye, values may be around -6.00 DC at 30º of retinal eccentricity. This means the peripheral retina has two main foci: the tangential represents the meridian that radiates out from the optical center, analogous to the spokes of a bicycle wheel; the sagittal represents that which is perpendicular to the tangential plane at any point. The tangential image plane falls in front of the sagittal image plane, so if the tangential image plane is focused on the retina the sagittal image plane falls behind the retina to act as a potential myopia growth signal, so ideally, we want the sagittal plane in focus so that the tangential plane falls inside the eye. We need more investigation on this, but it seems that having sagittal image on the retina may be helpful in determining the ideal peripheral plus power. Because oblique astigmatism acts like against-the-rule astigmatism we can use this to determine the best peripheral plus power by seeking the amount of peripheral plus that neutralizes off axis retinoscopy in the vertical meridian. When this is the case the horizontal tangential image plane will fall favorably inside the eye.
Two main higher order aberrations involved in optical quality are spherical aberration (SA) and coma. Both have been related to a possible myopia control effect - Hiraoka stated a relationship between higher coma values and myopia control effect in children wearing OK.4 Some attempts have been made to modify SA alone to control myopia5,6. Complicating the picture is the fact that by changing SA, accommodation is modified.7,8, Underaccommodation (lag) during near work is quantified as the difference between the dioptric level of the accommodative stimulus and the measured accommodative response. Larger lag in association with near work, which induces retinal blur, has been proposed as a factor in myopia development and progression9,10.
A reduction in lag of accommodation is seen using optical devices that change SA. Specifically, we found a significant reduction with the Soft RRG lens from 0.64±0.28 D to 0.37±0.42 D, link to abstract. Some studies investigating the link between accommodation and myopia progression, in particular with progressive addition spectacles, have shown promising results in children with rapid myopia progression, with higher success in patients with esophoria at near and higher accommodative lag.11 It seems plausible that reducing the higher accommodation lag seen in myopes could provide optimized retinal image characteristics. Visual contrast is greater when Zernike coefficients Z20 (defocus) and Z40 (primary SA) of the eye and lens system have opposite signs. A positive SA present in myopia control treatments such as OK and radial refractive gradient lenses combined with myopic peripheral blur has the potential to reduce the accommodation lag, placing the image plane in front of the retina,12 signaling the eye to stop growing. Because the amount of positive SA declines with accommodation and becomes steadily more negative with further accommodation13,14, in the myopic eye negative SA and peripheral hyperopic blur could push the image plane behind the retina, resulting in a higher accommodation lag, worsening the peripheral defocus and potentially inducing myopia. It seems plausible, then, that the increase in positive SA with a myopia controlling contact lens may protect against this situation.
Myopia control from the optical point of view is complex, but the good news is that new contact lens designs are on the way, and when we add peripheral plus power we are in fact modifying many optical factors which each may play a role in myopia control. The future is now, as we see this new visual care specialty developing for the clinician.
Meet the Authors:

About Jaume Paune Fabre
Jaume Paune Fabre is a clinical optometrist and contact lens designer from Barcelona, Spain who obtained his PhD in Optics and Optometry with the topic “Myopia control with radial refractive gradient contact lenses”. He holds two Spaniard National Council of Optics and Optometry awards along with several contact lens design patents, and in his spare time enjoys traveling, skiing and hiking.
References
- Smith EL. Prentice Award Lecture 2010: A case for peripheral optical treatment strategies for myopia. Optom Vis Sci. 2011;88:1029-1044. (link)
- Chiang ST-H, Phillips JR, Backhouse S. Effect of retinal image defocus on the thickness of the human choroid. Ophthalmic Physiol Opt.2015. (link)
- Loertscher M. Multifocal orthokeratology associated with rapid shortening of vitreous chamber depth in eyes of myopic children. Contact Lens Anterior Eye. 2013;36(2013):e2. (link)
- Hiraoka T, Kakita T, Okamoto F, Oshika T. Influence of Ocular Wavefront Aberrations on Axial Length Elongation in Myopic Children Treated with Overnight Orthokeratology. Ophthalmology.2014:1-8.(link)
- Parker KE, Marsack JD, Elswick JD, Brunstetter TJ, Applegate R a. Controlled induction of spherical aberration with custom soft contact lenses. Clin Exp Optom. 2009;92(3):283-288. (link)
- Cheng X, Chehab K, Brennan NA, Jingu X. Controlling myopia progression with positive spherical aberration in soft contact lenses. Optom Vis Sci. 2013;90(E-abstract 130252.) (link)
- Gifford P, Li M, Lu H, Miu J, Panjaya M, Swarbrick HA. Corneal versus ocular aberrations after overnight orthokeratology. Optom Vis Sci. 2013;90:439-447. (link)
- Tarrant J, Liu Y, Wildsoet CF. Orthokeratology Can Decrease the Accommodative Lag in Myopes. In: ARVO Meeting Abstracts.2009:4294. (link)
- Gwiazda JE, Hyman L, Norton TT, et al. Accommodation and related risk factors associated with myopia progression and their interaction with treatment in COMET children. Invest Ophthalmol Vis Sci. 2004;45:2143-2151. (link)
- Price H, Allen PM, Radhakrishnan H, et al. The Cambridge Anti-myopia Study: variables associated with myopia progression. Optom Vis Sci. 2013;90(11):1274-1283. (link)
- Berntsen DA, Sinnott LT, Mutti DO, Zadnik K, Group CS. Accommodative lag and juvenile-onset myopia progression in children wearing refractive correction. Vision Res. 2011;51:1039-1046. (link)
- Rosen R, Lundstrom L, Unsbo P, Lundström L, Unsbo P. Sign-dependent sensitivity to peripheral defocus for myopes due to aberrations. Invest Ophthalmol Vis Sci. 2012;53:7176-7182. (link)
- Cheng H, Barnett JK, Vilupuru AS, et al. A population study on changes in wave aberrations with accommodation. J Vis. 2004;4:272-280. (link)
- Atchison DA. Recent advances in measurement of monochromatic aberrations of human eyes. Clin Exp Optom. 2005;88:5-27. (link)
- Smith EL, Hung LF. Form-deprivation myopia in monkeys is a graded phenomenon. Vision Res. 2000;40:371-381. (link)
- Zhu X. Temporal integration of visual signals in lens compensation (a review). Exp Eye Res. 2013:69-76 (link)
Enormous thanks to our visionary sponsors
Myopia Profile’s growth into a world leading platform has been made possible through the support of our visionary sponsors, who share our mission to improve children’s vision care worldwide. Click on their logos to learn about how these companies are innovating and developing resources with us to support you in managing your patients with myopia.